

Dr. Farah Musharbash is a fellowship-trained spine surgeon at Atlantic Brain and Spine who treats cervical, thoracic, and lumbar spinal disorders. He specializes in minimally invasive and endoscopic spine surgery, adult and paediatric scoliosis, and advanced robotic and motion-preserving procedures, including disc replacement. He completed a combined Orthopaedic and Neurosurgery Spine Fellowship at the Hospital for Special Surgery (HSS), Weill Cornell, and Memorial Sloan Kettering in New York City. He completed his Orthopaedic Surgery residency at The Johns Hopkins Hospital in Baltimore and earned his medical degree from Washington University in St. Louis. He has authored more than 50 peer-reviewed papers including new techniques in endoscopic spine surgery and has received multiple awards including Patients Top Choice Award by U.S. News & World Report.
SSN: What drove you to choose surgery as a career – and spine surgery in particular?
FM: I was drawn to surgery because it combines technical skill, problem-solving, and a direct impact on patients’ lives. Spine surgery stood out because it sits at the intersection of function, pain, and quality of life. A spine condition can affect everything—how someone walks, sleeps, works, exercises, and interacts with their family.
What I find especially meaningful is the balance of precision and judgment. Not every patient needs surgery, and part of being a good spine surgeon is knowing when it will truly help—and when it won’t. I also enjoy the breadth of the field, from minimally invasive decompressions and motion-preserving procedures to complex deformity correction and paediatric conditions. It’s constantly evolving, which keeps it both challenging and rewarding.
SSN: You have developed significant clinical experience with robotic pars fracture repair in paediatric and adolescent patients. Can you tell us about your experience with this technique and how it relates to the emerging research in the field?
FM: Pars fracture repair is a very exciting area in spine surgery, particularly for younger patients and athletes, because it offers the ability to treat the source of pain while preserving motion. My focus has been on applying robotic technology to direct pars repair in carefully selected patients. As the highest-volume surgeon in New Jersey performing outpatient robotic pars repairs, I am currently studying my outcomes. We’re seeing that robotics can transform what was traditionally a more invasive procedure—often requiring 1-2 night hospital stays—into an outpatient surgery using small percutaneous incisions.
Patients are returning to sports as early as six to eight weeks post-operatively. While long-term comparative data is still evolving, robotics may improve reproducibility, shorten recovery, and maintain similar healing rates and long-term outcomes compared to traditional open techniques.


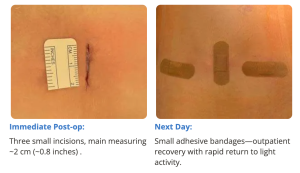
Images show pre-op CT and post-op CT, showing the healing, as well as a picture of the incisions. Image credits: Dr. Farah Musharbash
SSN: What could your findings and the use of robotic technology mean to help support spine surgery on paediatric patients and what will be the effect on patient experience and their recovery post surgery?
FM: Robotic technology has the potential to improve accuracy, efficiency, and consistency—especially in procedures requiring precise screw placement and trajectory planning.
In paediatric and adolescent patients, this can translate into a less invasive experience, smaller incisions, less tissue disruption, and potentially a smoother recovery. It also supports the broader goal of motion preservation, which is especially important for young, active patients.
From the patient and a family perspective, one of the biggest advantages is that, in appropriately selected cases, this can be done on an outpatient basis. The goal is not just to treat the injury, but to help patients safely return to school, sports, and normal life as efficiently as possible.
SSN: Regarding competitive athletes, what are the conservative non-operative options available for treating them against traditional surgical repair?
FM: Most athletes with pars stress injuries or fractures should begin with non-operative treatment. This typically includes activity modification, temporary cessation of aggravating sports, bracing, and physical therapy focused on core strength and mechanics, followed by a structured return-to-sport protocol.
This approach is successful in over 90% of cases. I consider surgery when symptoms persist despite appropriate conservative care, imaging correlates with the symptomatic pars defect, and the patient is a good candidate for motion-preserving repair rather than fusion.
SSN: Based on your clinical experience and the innovation happening in this area, what do you think the future looks like for the treatment of paediatric pars fracture?
FM: The future is moving toward more individualised, motion-preserving strategies. Historically, some patients were either braced for exceedingly long times or offered a fusion, but direct pars repair offers a different philosophy—addressing the problem while preserving the natural motion segment. Advances in robotics, imaging, and preoperative planning are making these procedures more precise and reproducible. At the same time, we’re improving our ability to identify which patients benefit most from non-operative care, repair, or in rarer cases – fusion. Stronger outcomes data will be key. My current research is part of that effort—helping define patient selection, recovery pathways, and return-to-sport timelines.
SSN: Do you have any more research in the pipeline?
FM: Yes. In addition to robotic pars repair outcomes, I am studying outcomes in endoscopic, motion-preserving techniques as well as adult and paediatric deformity surgery.
Over the next several years, some of the most important work will focus not just on whether new technologies are effective, but on which patients benefit most—and how we can use these tools to improve recovery and overall patient experience.
SSN: What are your thoughts on the advancing involvement of AI and 3D technology in surgery and patient care?
FM: AI and 3D technology will play a major role in the future of spine care. We’re already seeing how advanced imaging, navigation, and robotics improve surgical planning and precision.
The next step is using AI to support decision-making, identify patterns in outcomes data, and personalize treatment strategies. Three-dimensional visualization is also critical, as spine surgery relies heavily on anatomy, alignment, and spatial relationships.
That said, these tools should enhance—not replace—clinical judgment. The human side of medicine—listening to patients, understanding their goals, choosing the right treatment, and performing surgery thoughtfully—will always remain central. The best future is one where technology makes good surgeons even better and helps patients receive safer, more tailored care.
SSN: What’s the best part of your job?
FM: Seeing patients get their lives back. Many come in limited by pain and unable to do the things they enjoy. Helping restore that function—especially in young patients and athletes—is incredibly rewarding. I also enjoy the relationships that develop over time. Spine care is rarely just one conversation; it is a process of education, decision-making, treatment, and follow-up. Being able to guide patients and families through that process is one of the most meaningful parts of what I do.
SSN: … and the worst?
FM: When there isn’t a simple or immediate solution. Spine conditions can be complex, and not every patient improves quickly. In those cases, the most important thing you can offer is honesty, guidance, and a thoughtful, individualised plan.
SSN: What has been the highlight of your career so far?
FM: Thankfully I have had many highlights, and every patient story is meaningful. One was performing an emergency surgery on a young patient who was paralysed from a spontaneous epidural hematoma and seeing him walk into my office unassisted two weeks later. Another was a 15-year-old athlete going home the same day after robotic pars repair—and later returning to soccer within three months. Those moments are incredibly meaningful.
SSN: Are you planning to attend or speak at any medical conferences or events in 2026?
FM: Yes, I’ll be speaking at the ISASS conference in Miami this April and at the HSS Summer Reunion in the Hamptons in August. I’ll also be attending the State of Spine Surgery Think Tank in Cabo, along with other meetings throughout the year.
Text and images supplied by the author
